One of the major criticisms of the theory that the Inverted W -- and the other inverted arm actions -- is bad is that it hasn't been directly studied. Instead, up to this point I have had to rely on studies of general pitching mechanics to back up my claims.
That is no longer the case.
2012 Poster
In 2012 Dr. Weimi Douoguih, Medical Director for MedStar Sports Medicine and Medical Director for the Washington Nationals, commissioned a study that looked at my claims with respect to the Inverted W. He did this by looking at the pitching mechanics of major league pitchers during the 2010 and 2011 seasons and comparing their pitching mechanics, arm action, and timing to their injury histories.
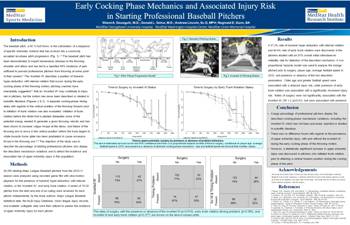
Early Cocking Phase Mechanics
and Associated Injury Risk
The study found statistically significant evidence that backs up my assertions.
Lets go over some of the key aspects of that study and examine their relevance and importance.
Methods
All 250 starting Major League Baseball pitchers from the 2010-11 season were analyzed using recorded game film with slow-motion playback for the presence of humeral hyper-abduction with internal rotation, or the ‘inverted W’, and early trunk rotation. A series of 15-20 pitches from the start and end of an outing were reviewed for each pitcher independently by the study authors. Major League Baseball statistical data, the MLB Injury Database, minor league injury records, and available collegiate data were then utilized to assess the incidence of upper extremity injury for each pitcher.
Results
A 37.2% rate of humeral hyper-abduction with internal rotation and 44.4% rate of early trunk rotation were discovered in the pitchers studied with an 87% overall initial inter-observer reliability rate for detection of the described mechanics. A Cox proportional hazards model was used to analyze the innings pitched prior to surgery, player age, average fastball speed in 2010, and presence or absence of the two described parameters. Older age and greater fastball speed were associated with a reduced injury risk, while presence of early trunk rotation was associated with a significantly increased injury risk. Rates of surgery were not significantly associated with the inverted W, OR 1.2 (p=0.61), but were associated with presence.
Conclusion
A large percentage of professional pitchers display the described cocking-phase mechanical variations, including the inverted W, which has not been previously reported or studied in scientific literature.
There was no difference found with regards to the prevalence of upper extremity injury, with and without the inverted W, during the early cocking phase of the throwing motion.
However, a statistically significant increase in upper extremity injury was discovered in pitchers who initiated trunk rotation prior to attaining a vertical forearm position during the cocking phase of the pitch.
In other words, and as I have been saying for years, the problem with the Inverted W isn't the position itself. Rather, the problem with the Inverted W is its impact on a pitcher's Timing.
By hurting a pitcher's timing, the Inverted W can contribute to injury problems to both the elbow and the shoulder.
2015 Paper
Dr. Douoguih recently release the full study of the Inverted W off of which the poster above was based, and I am working on an analysis of the Douoguih study of the Inverted W.